ABSTRACT
Management of infectious diseases in remote nomadic communities is a problematic affair because these people are mobile, geographically isolated, and have limited access to health facilities. This review will address diagnostic and predictive disease modeling systems among people on the move using Geographic Information Systems (GIS). It analyses how GIS has been used in controlling and surveilling the diseases among the nomads by examining 22 selected peer-reviewed studies. It also aims to demonstrate how GIS is used in health informatics in terms of analyzing mobility and health and disease diffusivity in high-risk groups.
The promising usage of GIS in terms of healthcare is proposed, such as the ones concerning spatial epidemiology and disease diffusivity/mobility interactions modeling, mobile health integration, and monitoring of health technologies. However, collecting data in remote regions, health technology infrastructure, and spatialization of health of populations on the move over time are all impressive obstacles. This paper underlines the necessity to develop models of mobile, distant supervision networks and culturally adapted data collection procedures and Nomadic movements due to climatic change.
INTRODUCTION
The nomadic, along with semi-nomadic population, will be the hardest group of people to apply disease surveillance and control measures to them and a rough estimate of 200 to 500 million is the number of people that they represent. Examples of such marginalized populations in sub-Saharan Africa, Central Asia, e.g., Pakistan such as Pakistan, and mobile peoples in war zones. These individuals endure medical conditions such as illnesses as a result of mobility cycles and inability to access medical services, in addition to the variable climatic conditions they are exposed to [1]. Surveillance systems implemented to watch fewer active populations are ineffective in tracking mobile communities, and this should not be a concern in addressing global health security gaps [2].

The diversity of nomadic lifestyles is often characterized by the frequent movement across political boundaries, migration paths, although they come into contact with various ecosystems, which complicates disease modeling due to the nature of having to live multiple types of lifestyles: this is what makes disease modeling a complicated process for nomadic lifestyles, unique to this challenge [3]. GIS, with its ability to track the movement of people, model the spread of diseases across various geographies, and aggregate various types of information into a single surveillance window, has become essential toward solving [4] these problems. The newest GIS technologies make it possible not only to monitor the outbreaks of diseases, but also to trace the human activity ecosystems, and disease relationships on various spatial and temporal scales by using satellite images, GPS, and other additional data [5].
GIS technology is not being used quite in the same fashion to monitor health in nomadic populations as it is in sedentary populations and it faces other challenges that include slow internet service in hard to get to areas, the need to travel with local community roles, and the complexity of the mobility of a population that makes modelling the transmission of disease quite tricky [6]. Despite these obstacles, the emerging mobile GIS, community-based surveillance systems, and participatory mapping tools have all been promising in meeting the The ISSN 2326-23032 / 3 2023 International Journal of Scientific Research and Management extends to surveillance of diseases in nomadic populations through the use of technology to address the health inequities.
In the present literature review, the health inequities phenomenon is discussed as being rife and requiring exact targeting. Health surveillance is an important aspect of medicine and literature review, the authenticity of data, the systems present, and in tandem with the health system that is in use, and the evaluative potential of human resources in the assessment process. It is anticipated that through this literature review, we will be able to provide evidence-based strategies ready to redesign health systems in place, shift engagement inequity, TARGET mobile populations, and their mobility patterns. The purpose of the conclusion is to discuss health surveillance systems that are better than disease surveillance and control systems in terms of disease control, in addition to.
STUDY AREA
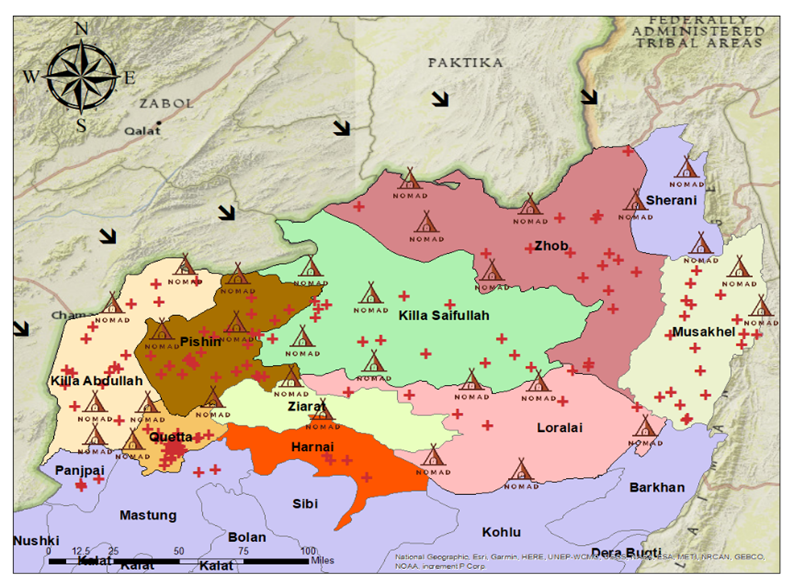
To fill the void of empirical data, in order to complement the findings found in the literature, a field survey was carried out with nomadic communities in Balochistan’s districts such as Killa Saifullah, Pishin, Killa Abdullah, Zhob, Loralai, Musakhel, Sherani, Harnai and Quetta Pakistan. The need to conduct on-the-ground research played an important role in anchoring the study in the reality of the population. The available primary data became the main source to validate the theoretical modelling and the issues faced in the literature.
The team also directly involved nomadic populations by using a mixed-method approach in data collection methods to obtain comprehensive data on mobility, health, and their environment. It also involved face-to-face answering of questions, which aimed to note and record qualitative information on how people seek health, what illnesses are prevalent, and how the culture thinks of technology and healthcare. In resolving the underlying issue of population mobility, GPS systems were applied to carefully chart the seasonal population movements of the communities. This gave accurate geospatial data relating to their movement patterns, and this is a critical variable to model the spread of disease. Also, there was an observational appraisal of the situation on the ground, evaluating aspects of clean water, sanitation, and possible disease carriers to give a geographical underpinning to the health statistics.
The information from the field survey, such as the field mapping in terms of routes by GPS and health observations, was integrated into a GIS-based framework. This was a key innovation in the context of the study, since it resulted in the development of a unique dataset, not only allowing the visual and analytical connection of population movement and health outcome, but also enabling the examination of health outcomes by migration control in a way that had never been done before. Through overlaying the collected information, the study flared above the theoretical models and was able to come up with a more realistic and data-informed set of illustrations of the disease diffusivity in nomadic populations. This empirical evidence was critical to enhancing the conclusions made in the study and developing a foundation based on the cultural and logistical conditions of nomadic living that are sensitive to evidence-based suggestions.
MATERIAL AND METHODS
The collective of research was literally on track with asking nomads, as they were dealing with human participants directly, and employing a mixed-method data collection strategy:
GPS-Based Route Mapping: The seasonal migration route and mobility patterns were more effectively mapped through GPS devices and enabled the measurement of distance between each point. This geospatial information played a critical role in the modelling of the dynamics of disease spread.
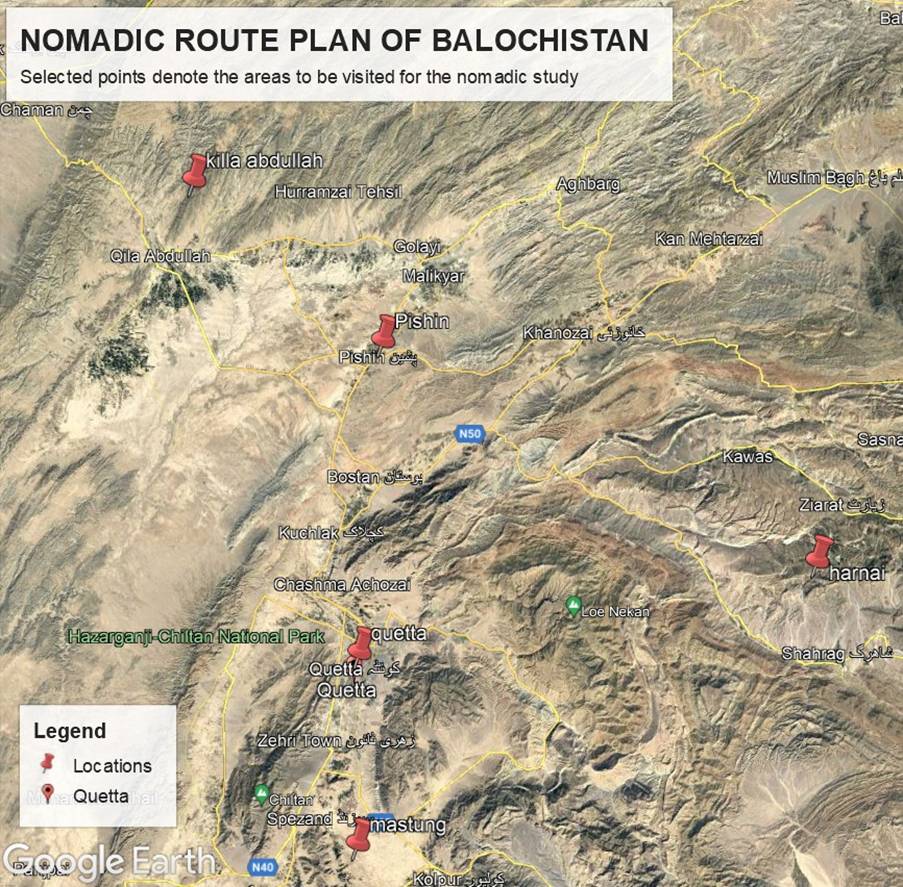
Figure 5 selected regions of nomads movement routes due to climatic change
Direct observations have also been used in evaluating the living and the environmental and climatic situations, such as sanitation, water supplies, and potential disease carriers, which gave context to the health data obtained.
Face-to-face interviews: To collect qualitative data about the community health issues, access to healthcare, and the cultural settings of health practice, a structured and semi-structured interview was conducted in Cold climate region of Balochistan.

A number of challenges and limitations have been adequately covered in this review. The most pronounced obstacles are cultural resistance, technical complexity, limitations to resources, data collection, and connectivity and infrastructure problems. The application of sophisticated GIS in nomadic settings is doomed to failure because of remoteness and limited access to infrastructure [19].
Another significant barrier is the cultural complexity of work with nomadic communities, which requires engagement with the community, culturally sensitive methods of cooperation, and slow-paced trust-building. Moreover, since nomadic populations are dynamic, they might not be captured completely by conventional epidemiological mechanisms, considering that the nature of the nomadic groups is continuously on the move due to climate change and challenges of healthcare [20]. This poses a unique methodological difficulty for disease modeling.
The importance of the nomadic health surveillance goes beyond the health surveillance effort, but it raises a recommendation to other health equity efforts around the globe [21]. As an example, GIS practices with nomadic communities may be modified to accommodate other vulnerable groups, such as internally displaced persons, refugees, and seasonal laborers. What has been learnt through nomadic disease surveillance can provide a guide to using geospatial technologies in the context of other health equity interventions designed to reach underserved populations [22].
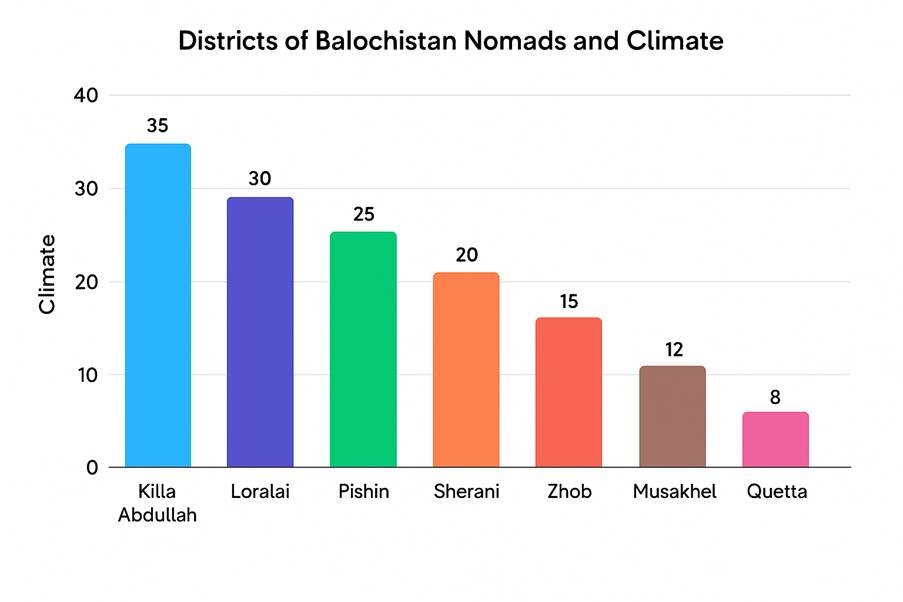
Figure 7 Nomadic Population District wise, Balochsitan
CONCLUSION
The use of GIS in epidemiological surveillance in nomadic populations has revolutionized the process and formed a substantial platform in terms of overcoming global health equity disparities and enhancing international health security due to climate chnage. GIS technology is able to streamline disease tracking systems, observe population flows and health data, and pinpoint at-risk groups, especially in hard-to-reach regions and in conflict regions.
Various advances should be pursued in the full realization of the promise of GIS in the engagement of health equity. These involve developing a powerful mobile-based information collection system, establishing an all out thorough, culturally acceptable training program to close the technical expertise skill gap among the local health workers, and the establishment of a powerful community partnership program to overcome the sociocultural barriers.
Standard data-sharing frameworks developed specifically to support the unique needs of mobile populations, coupled with investments into offline-capable mobile health applications that enable monitoring at the community level, have the potential to allow most of the lessons learned in nomadic disease surveillance to be transferred to other disadvantaged groups. The above improvements, combined with an extended commitment to proper technology infrastructure and community involvement, will not only enhance equitable health surveillance systems but will also aid the objectives of universal health coverage and international health security.